Endonasal Endoscopic CSF Leak Repair: Trans-Cribriform and Transpterygoid Approach
Ramakrishnan V1, Soumya C V2
- Senior Consultant, Department of Otolaryngology-Head and Neck Surgery, Aster-Mims Kannur, Kerala;
2. Senior consultant, Department of Neurology, Aster-Mims Kannur, Kerala.*
Corresponding Author: Dr Ramakrishnan V, MS (ENT), DNB (ENT)
Senior Consultant ENT Surgeon, Aster-MIMS Kannur.
Email: joshrama@yahoo.com
Background: Cerebrospinal fluid (CSF) leak which occurred in the left cribriform plate and the left lateral recess of sphenoid sinus in a middle aged woman which was idiopathic in origin. This observation aims to report a case of endoscopic repair of the defects through the transcribriform and transpterygoid route in the same sitting.
Case Report: A 41 year old middle aged woman was referred from the department of neurosciences to the department of ENT with a watery discharge from the left nasal cavity and on evaluation bony defects were identified in the left cribriform plate and the left lateral recess of sphenoid with meningoencephalocele. The leak was repaired using the endoscopic transcribriform and the transpterygoid approach. The surgical procedure was uneventful.
Discusssion: Endoscopic transcribriform and transpterygoid approaches were utilized in closing the defects. The defect in the left cribriform plate was sealed after bipolar coagulation with fat, fascia lata and tissue glue and the lateral recess of sphenoid defect was closed with fat, artificial dura, fascia lata and tissue glue and the patient recovered successfully after the procedure.
Keywords: Cerebrospinal Fluid Leak, Lateral Recess of Sphenoid, Transcribriform and Transpterygoid
Introduction
Cerebrospinal fluid rhinorrhoea results from the disruption in the barriers between the sinonasal cavity and the anterior and middle cranial fosaa leading to discharge of csf into the nasal cavity.5 Cerebrospinal fluid leak is a rare condition that leads to a multitude of infectious complications and impart significant morbidity and potentially disastrous long term deficits for the patient.10,16 CSF leak is caused by trauma in 80-90 percent of cases and non traumatic in 4-10 percent of cases of which 14-55 percent are idiopathic in non traumatic situations.16,11 A csf leak in the cribriform plate and the lateral recess of sphenoid can be repaired in the same sitting through the transcribriform and the transpterygoid route.17,18 The aim of the surgery is to seal the defect in the anterior and middle skull base,which, if left untreated has an increased risk of ascending intracranial infections.5 In addition this restores brain buoyancy and prevents CSF hypotension.5
Case report
A 41 year old woman complained of watery discharge from the left nasal cavity for the past 6-8 months while presenting at the out patient department of our institute. The watery discharge was spontaneous in onset, intermittent initially and thereafter almost continuous at times, increasing when the patient was sitting leaning forward, during head down positions, during straining and was tasting salty. There were no complaints of nasal obstruction, nasal pain or olfactory discturbances. However the patient used to complaint of headaches intermittently but without any meningitis features as evaluated by the neurologist (second author). No abnormality was found in the right nostril. Nasal endoscopy revealed clear fluid discharging from the left nasal cavity which positive for sugars and beta-2 transferrin.
CT cisternography revealed thinning and erosion of the left cribriform plate posterior to the crista galli (figure 1) and the lateral recess of the left sphenoid (figure 2).
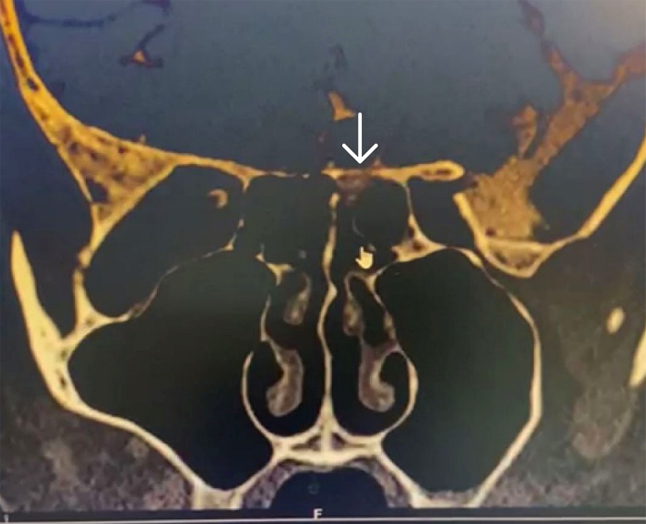
Figure 1. CT cisternography -arrow showing thinning and erosion of the left cribriform plate posterior to the crista galli showing csf leakage
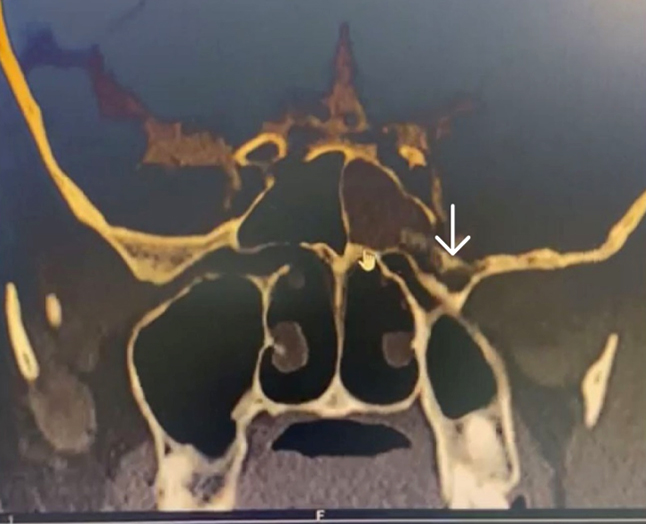
Figure 2. CT cisternography -arrow showing thinning and erosion of the lateral wall of sphenoid sinus above vidian-rotundum line with csf leakage
MRI brain with anterior skull base revealed protrusion of the anteromedial left temporal lobe in to the left sphenoid sinus which was hyperintense on T2 and normal on T1 and FLAIR sequences suggestive of encephalocele (figure 3). The left gyrus rectus shows inferior elongation with no definite encephalocele at the cribriform site (figure 3A).
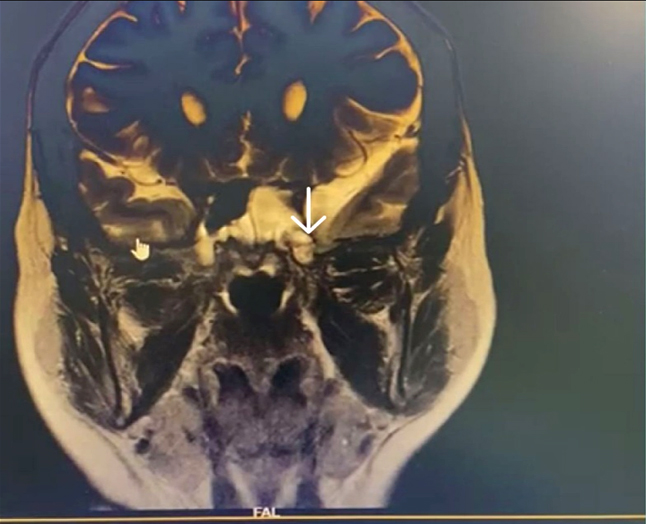
Figure 3. MRI brain with skull base –normal signal on T1 and FLAIR with hyperintense on T2 signifying protrusion of the anteromedial temporal lobe with left meningoencephalocele.
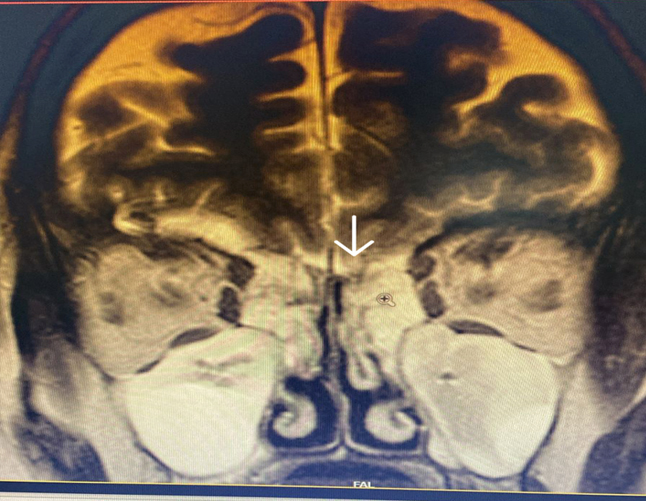
Figure 3A. MRI brain with anterior skull base -left gyrus rectus abnormal inferior elongation (at the CSF leak site on cisternography with no definite encephalocele
The surgery was performed under general anaesthesia by the first author. Nasal endoscopic examination after administering general anaesthesia showed watery discharge from the region of the left cribriform plate (figure3 B) and the left spheno-ethmoidal recess (figure 4). The surgery proceeded with left partial middle turbinectomy and widening of the sphenoid ostium on the left side. This was followed by left uncinectomy, middle meatal antrostomy, left anterior ethmoidectomy an removal of basal lamella and posterior ethmoidectomy. This was followed by clear delineation of the leak in the left cribriform plate and a wide sphenoidotomy (figure 5). The edematous sphenoid sinus mucosa was removed and the meningoencephalocele was seen in the left lateral recess above the vidian-rotundum line. The sphenoplalatine foramen was identified and the sphenopalatine artery cauterized. The medial aspect of the posterior wall of left maxillary sinus was removed partially. The upper part of the pterygoid process was drilled out and widened laterally exposing the antero-medial temporal lobe and the meningoencephalocele (figure 6) and the continuous csf leak leak identified.
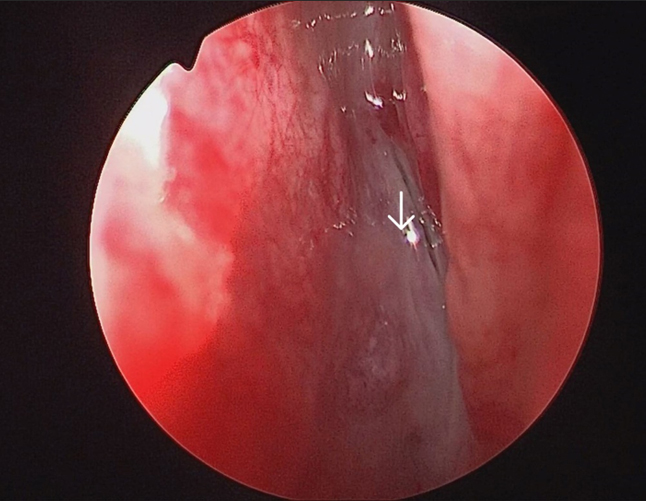
Figure 3B. Arrow showing leak in the left cribriform plate
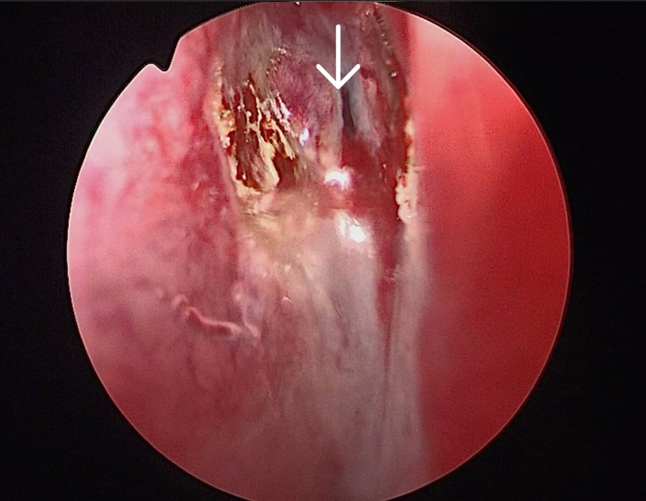
Figure 4. Arrow showing csf leak in the left sphenoethmoidal recess
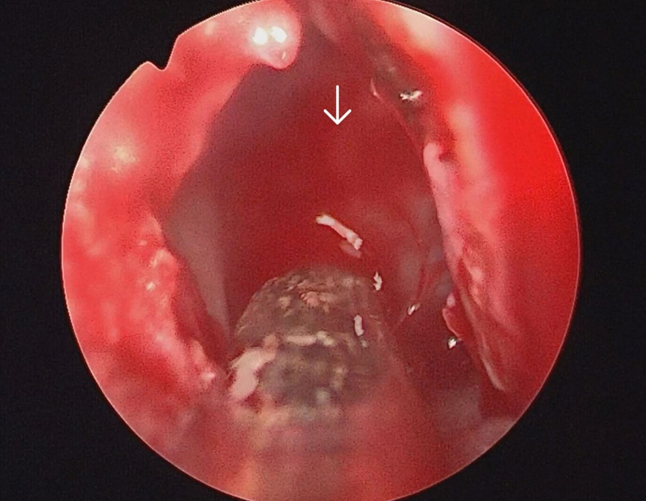
Figure 5. Arrow showing csf gusher in the left sphenoid sinus after endoscopic left sphenoidotomy.
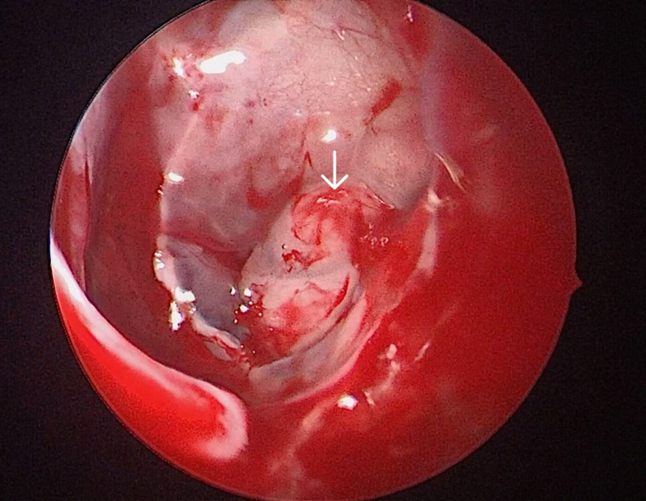
Figure 6. Arrow showing the meningoencephalocele in the left lateral recess of sphenoid with csf leak through the defect
The meningoencephalocele was reduced by bipolar cauterization, the sphenoid sinus mucosa removed, the defect was closed by insertion of fat harvested from the left thigh (figure 7), followed by artificial dura, fascia lata harvested from the left thigh, followed by tissue glue and by another layer of fascia lata (figure 8). The defect in the cribriform plate was cauterised and sealed with fat and fascia lata harvested from the left thigh and subsequently reinforced with tissue glue and gel foam (figure 9).
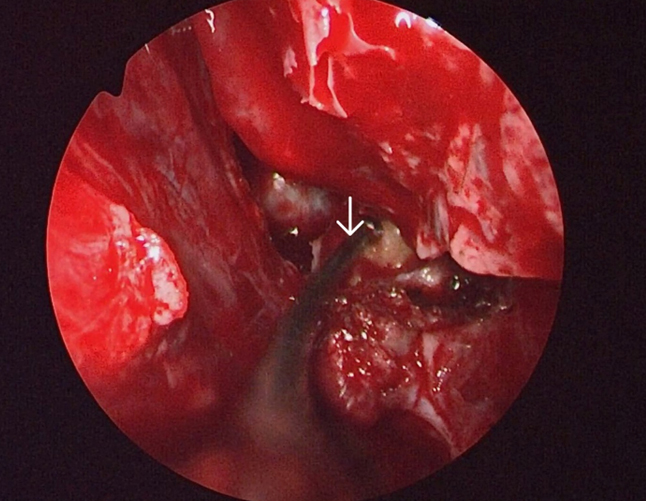
Figure 7. Arrow showing the fat being placed on top of the sealed defect of the left lateral recess of sphenoid
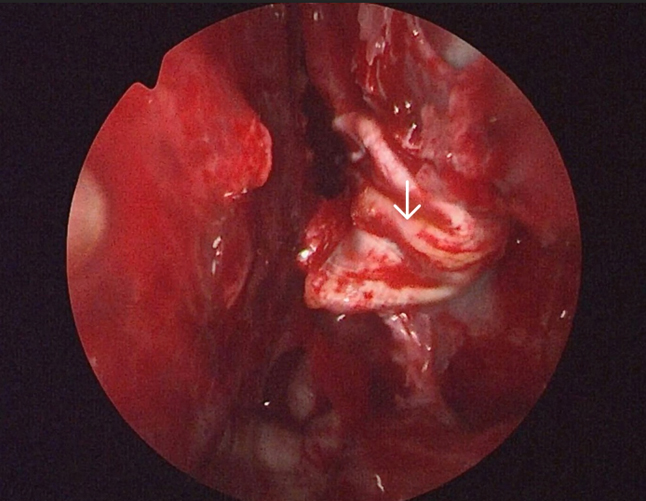
Figure 8. Arrow showing fascia lata being draped on the fat-artificial dura layers for reinforcement of the defect
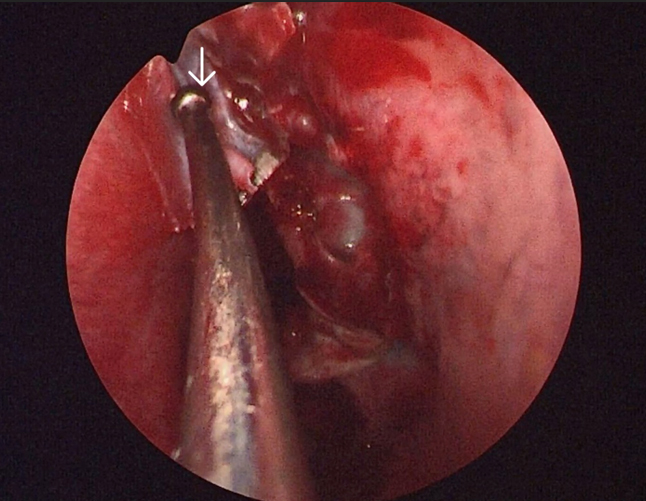
Figure 9. Arrow showing the fascia lata being place over the fat layer to seal the defect over the left cribriform plate
On table completion of the surgery showed no leaks from both the sites with a loss of blood of around 120ml. Post operatively she was put on a lumbar drain for a period of 3 days along with inj cefoperazone-sulbactum 1.5gm twice daily, laxatives, bed rest with head end elevation of 30 degrees for 5 days. The patient was discharged on the fifth post operative day with tab cefpodoxime 2oomg and tab acetazolamide 25omg twice daily for 10 days. The patient was advised not to strain, lean forward, lift weights for 3 weeks and to avoid sneezing and coughing. Nasal endoscopy 3 months after surgery showed a complete uptake of the graft with no evidence of any leak (figure 10).The patient is on follow up monthly for 18 months till now and is currently symptom free.
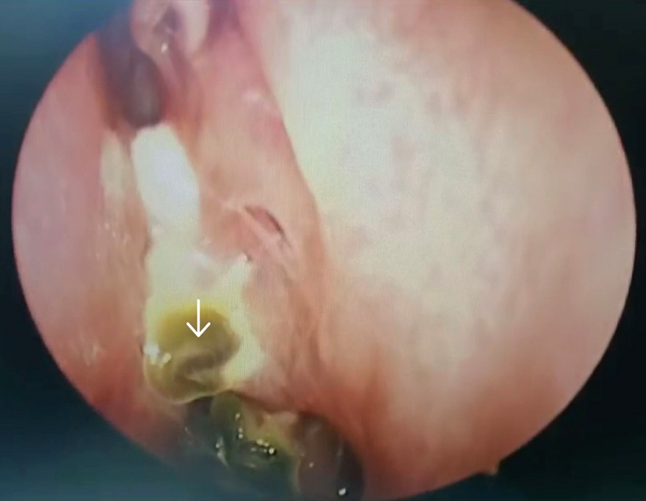
Figure 10. 3 months post operative view showing well taken up graft over the skull base with no csf leak
DISCUSSION
A csf leak in the lateral recess of sphenoid sinus is suspected to be due to a congenital abnormality of the dehiscence of the sternberg’s canal and the leak in the cribriform plate could due to raised intracranial tension.1 The etiology of csf leaks in general include congenital, tumour-related, traumatic and idiopathic. Non-traumatic leaks are more common in adult middle aged women, with a ratio of 1:2 for men and women.6 A csf leak can occur at any location, including defects in the frontal sinus 10 percent, anterior ethmoid 18 percent, lamina cribrosa 35 percent, sphenoid sinus 26 precent and inferior clivus 2 percent.15,6 Csf rhinorrheoa can be intermittent or continuous depending upon the size of the defects.
The clinical conformation of csf rhinorrheoa includes the observation of clear watery discharge from the left nostril on leaning forward followed by conformation of raised sugar levels and beta-2 transferrin levels in the nasal discharge.6 Nasal endoscopy can reveal the site of the leaks in the out patient department. CT cisternography was the investigation done in this case to confirm the leak as well as the sites.MRI brain and anterior skull base was also done to evaluate the meningoencephaloceles.MR cisternography is also being used as an investigative modality in select cases to assess leaks, vascular issues and plan surgeries accordingly. MRI brain and skull base can also be used to corroborate the findings including the evaluation of potential meningoencephaloceles.
Tumours, raised intracranial pressures, trauma and congenital skull base defects contribute of leaks in general especially sphenoid sinus (9.8 percent) in certain studies13,4 and other regions of anterior skull base like the cribriform plate. The main complication of persistent leaks is meningitis.13 Endoscopic transnasal transpterygoid approach for lateral recess defects is a highly successful approach with minimal morbidity and the endoscopic transcribriform approach for cribriform plate leaks has become the standard operating approaches with more than 90 percent success rates.7 The approach involves a middle turbinectomy, middle meatal antrosomy, anterior and posterior ethmoidectomies, sphenopalatine artery coagulation followed by drilling the left pterygoid exposing the lateral recess and assessment of the meningoencephalocele by correlating with the vidian-rotundum line. with the vidian-rotundum line7,13 along with delineation of the cribriform defect followed by cauterization of the leak site thereby sealing the defect. The sphenoid sinus mucosa in removed with a blakesley forceps in order to expose the lateral recess defect clearly ,and scraping the mucosa around the region of the cribriform plate to seal the leak site perfectly with absolute graft adhesion.13 Coablation can also be used to cauterize the defect sites. The defect can be covered with fat, fascia (fascia lata) in this case along with artificial dura and tissue glue13,4 (Figure 8).
Post operatively bed rest with head end elevation and lumbar drains for a couple of days to control the intracranial pressure along with antibiotics, carbonic anhydrase inhibitors, stool softeners ensures an uneventful recovery with high percentage of graft uptake.4,9
CONCLUSION
This is a case report/observation of a 41 year old woman with csf leak from the left cribriform plate and left lateral recess of sphenoid who underwent endoscopic endonasal transcribriform and transpterygoid closure of the defects using multi -layer reninforcements with fat, fascia lata, artificial dura, gel foam with final sealing with tissue glue. The patient was followed up regularly every month for the past 18 months with no leak on follow up nasal endoscopy with perfect skull base reconstruction.
END NOTE
Author information
- Dr Ramakrishnan V, MS (ENT), DNB (ENT)
Senior Consultant, Department of Otolaryngology-Head and Neck Surgery,
Aster-Mims Kannur, Kerala-670621.
Emial: joshrama@yahoo.com. - Dr Soumya C V, MD, DM, DNB
(Neurology), FRCP
Senior Consultant, Department of Neurology,
Aster -Mims Kannur, Kerala -670621.
Emial: soumya0@yahoo.com
Conflict of Interest: None declared
REFERENCES
- Martin-Martin C, Martinez-Capoccioni G, Serramito-Garcia R, Espinosa-Restrepo F. Surgical challenge: endoscopic repair of cerebrospinal fluid leak. BMC Res Notes. 2012;5:459.
[PubMed] | [Crossref] - El-Tarabishi MN, Coden E, Russo F, Elhassan HA, Gallo S, et al. Endoscopic endonasal transpterygoid approach to sphenoid sinus lateral recess defects. J Neurol Surg B Skull Base. 2020;81(5):553-561. [PubMed]
[Crossref] - Janakiram TN, Subramaniam V, Parekh P. Endoscopic endonasal repair of sphenoid sinus cerebrospinal fluid leaks: our experience. Indian J Otolaryngol Head Neck Surg. 2015;67(4):412-416.
[PubMed] - Oakley GM, Orlandi RR, Woodworth BA, Batra PS, Alt JA. Management of cerebrospinal fluid rhinorrhoea: an evidence-based review with recommendations. Int Forum Allergy Rhinol. 2016;6(1):17-24.
[PubMed] | [Crossref] - Virk JS, Elmiyeh B, Saleh HA. Endoscopic management of cerebrospinal fluid rhinorrhoea: the Charing Cross experience. J Neurol Surg B Skull Base. 2013;74(2):61-67.
[PubMed] | [Crossref] - Kim-Ordon N, Shen J, Or M, Hur K, Zada G, Wrobel B. Endoscopic endonasal repair of spontaneous cerebrospinal fluid leaks using multilayer composite graft and vascularized pedicled nasoseptal flap technique. Allergy Rhinol (Providence). 2019;10:2152656719888622.
[PubMed] | [Crossref] - Schmidt RF, Choudhry OJ, Raviv J, Baredes S, Casiano RR, Eloy JA, et al. Surgical nuances for the endoscopic endonasal transpterygoid approach to lateral sphenoid sinus encephaloceles. Neurosurg Focus. 2012;32(6):E5.
[PubMed] | [Crossref] - Kita AE, Bradbury DW, Taylor ZD, Kamei DT, St John MA. Point-of-care cerebrospinal fluid detection. Otolaryngol Head Neck Surg. 2018;159(5):824-829.
[PubMed] | [Crossref] - Fyrmpas G, Konstantinidis I, Selviaridis P, Constantinidis J. Management of spontaneous cerebrospinal fluid leaks of the sphenoid sinus: our experience. J Laryngol Otol. 2014;128(9):797-802.
[PubMed] | [Crossref] - Keshri A, Jain R, Manogaran RS, Behari S, Khatri D, Mathialagan A. Management of spontaneous CSF rhinorrhoea: an institutional experience. J Neurol Surg B Skull Base. 2019;80(5):493-499.
[PubMed] | [Crossref] - Englhard AS, Volgger V, Leunig A, Messmer CS, Ledderose GJ. Spontaneous nasal cerebrospinal fluid leaks: management of 24 patients over 11 years. Eur Arch Otorhinolaryngol. 2018;275(10):2487-2494.
[PubMed] | [Crossref] - Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A. The SCARE 2020 guideline: updating consensus surgical case report (SCARE) guidelines. Int J Surg. 2020;84:226-230
[PubMed] | [Crossref] - Spina A, Boari N, Calvanese F, De Domenico P, Cannizzaro M, Trimarchi M, et al.
Transcranial extradural subtemporal repair for sphenoid sinus lateral recess meningoencephalocele: technical note. Neurosurg Rev. 2021.
[Crossref] - El-Tarabishi MN, Fawaz SA, Sabri SM, El-Sharnobi MM, Sweed A.
Modification of endoscopic endonasal approach for management of encephaloceles in sphenoid sinus lateral recess. Eur Arch Otorhinolaryngol. 2016;273(12):4305-4314.
[PubMed] | [Crossref] - Lobo BC, Baumanis MM, Nelson RF.
Surgical repair of spontaneous cerebrospinal fluid leaks: a systematic review. Laryngoscope Investig Otolaryngol. 2017;2(5):215-224.
[PubMed] | [Crossref] - Dai JB, Del Signore AG, Govindaraj S, Bederson JB, Iloreta AMC, Shrivastava R. Investigation of skull base cerebrospinal fluid leak repair: a single-institution comprehensive study of 116 cases over 10 years. World Neurosurg. 2020;135:e1-e11.
[PubMed] | [Crossref] - Alexander NS, Chaaban MR, Riley KO, Woodworth BA.
Treatment strategies for lateral sphenoid sinus recess cerebrospinal fluid leaks. Arch Otolaryngol Head Neck Surg. 2012;138(5):471-478.
[PubMed] | [Crossref] - Mona MM, Sutkino B. Management of cerebrospinal fluid leak in the lateral recess of the sphenoid with transpterygoid approach: a case report. Int J Surg. 2021;89:106594.
[Crossref] - Abuzayed B, et al. Duraplasty using autologous fascia lata reinforced by on-site pedicled muscle flap: technical note. J Craniofac Surg. 2009;20(2):435-438.
[PubMed] | [Crossref] - He C, et al. Management of cerebrospinal fluid rhinorrhoea in the sphenoid sinus lateral recess through an endoscopic endonasal transpterygoid approach with obliteration of the lateral recess. Ear Nose Throat J. 2022;101(5):319-325.
[PubMed] | [Crossref]